
2024
AUMC: Service Design Recommendations for Clinical Workflow in a Cardiovascular Intervention Center
Categories:
Health & Care
Design Research
The Challenge
The Cardiovascular Intervention Center at Amsterdam UMC was transitioning to same-day admissions and an expanded facility: more procedure rooms, higher patient volume, faster turnaround. The coordination model that existed relied heavily on clinical staff manually tracking patients across stages, calling between units, and absorbing disruptions when emergency cases bumped the schedule.
Through on-site observations and interviews with nurses, a project leader, and Epic developers, three core problems emerged:
Coordination was reactive: staff responded to disruptions rather than anticipating them
Patient status was invisible: no shared view of who was where in the flow, for staff or families
Cognitive load was concentrated: clinical staff tracked everything manually while also delivering care
How might we design coordination tools that support nurses in focusing on care, not physical and informational logistics?
Approach
Rather than optimizing a single touchpoint, we analyzed the system as a whole.
Work system analysis mapping 15+ roles across tools, tasks, and environment, revealing where coordination gaps sit between people and systems.
SEIPS model (Systems Engineering Initiative for Patient Safety) mapped how people, tasks, tools, and environment interact, and where they break down. It revealed that the real problem was not any individual tool or person, but the gaps between them.
Patient Journey (using Metro-Mappaing method) traced the full patient experience from pre-visit through discharge, surfacing operational bottlenecks and emotional moments simultaneously. Comparing current and future-state journeys showed where the new same-day admission model would create new pressure points, not just resolve old ones.
Research included stakeholder interviews with nurses, a planning coordinator, and Epic developers; on-site observation in the short-stay and intervention units; and desk research on cardiovascular care workflows in the Dutch healthcare system.
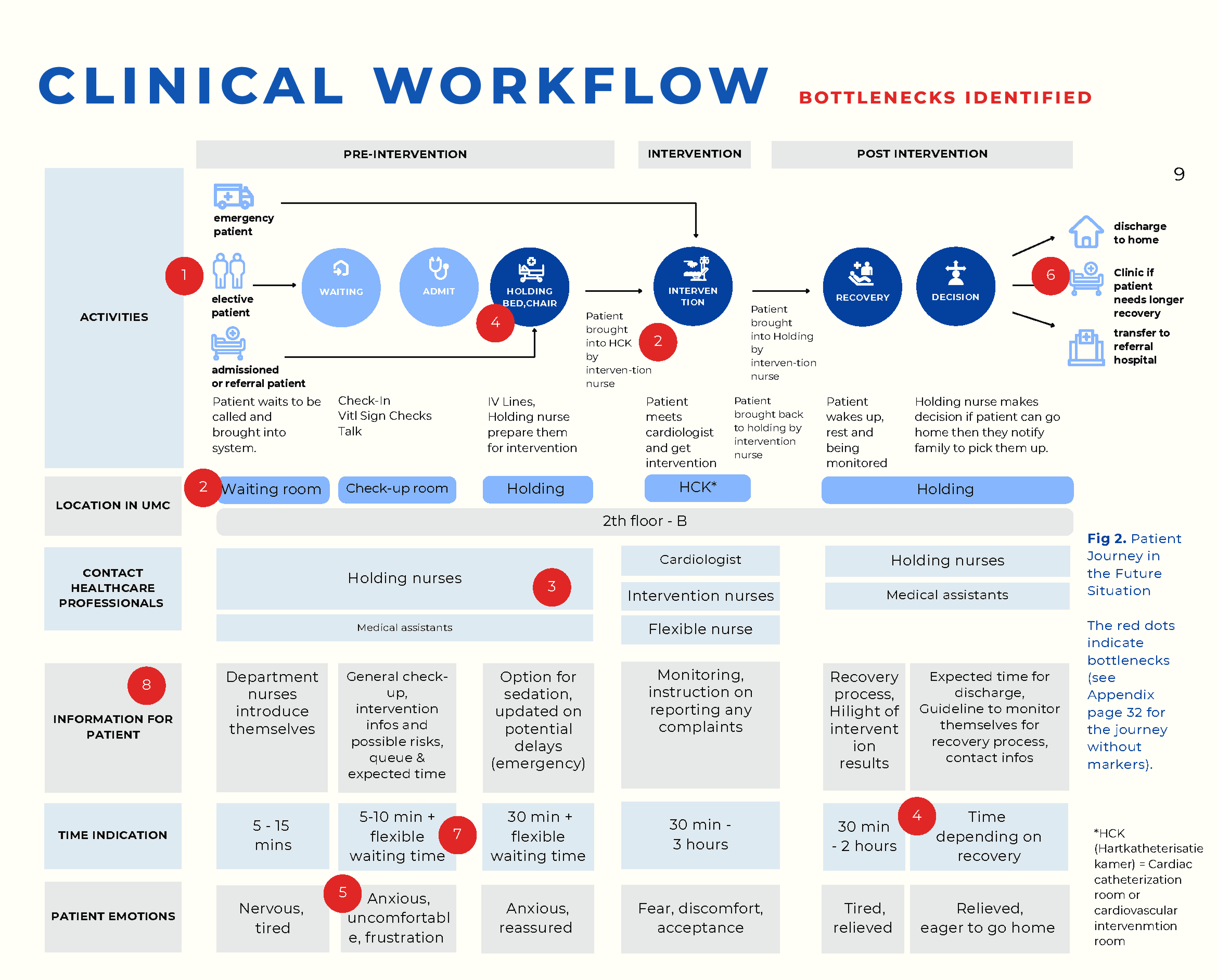
Future-state patient journey mapped across activities, locations, staff contact points, and patient emotions. Red dots mark eight bottlenecks — most cluster around holding, status visibility, and family communication.
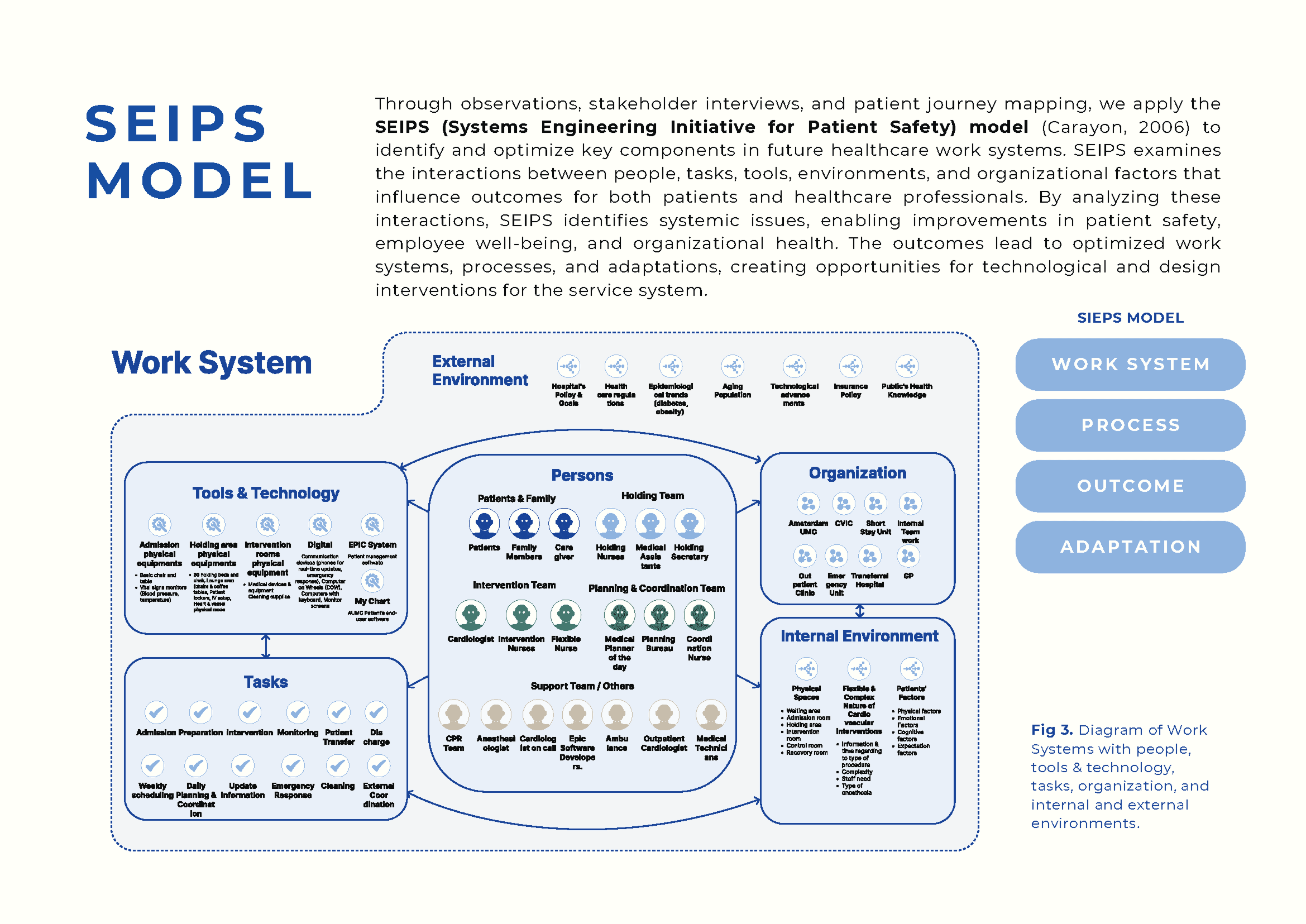
Work system analysis mapping 15+ roles across tools, tasks, and environment, revealing where coordination gaps sit between people and systems, not within them.
Research included stakeholder interviews with nurses, a planning coordinator, and Epic developers; on-site observation in the short-stay and intervention units; and desk research on cardiovascular care workflows in the Dutch healthcare system.
What We Did
Identified key pain points
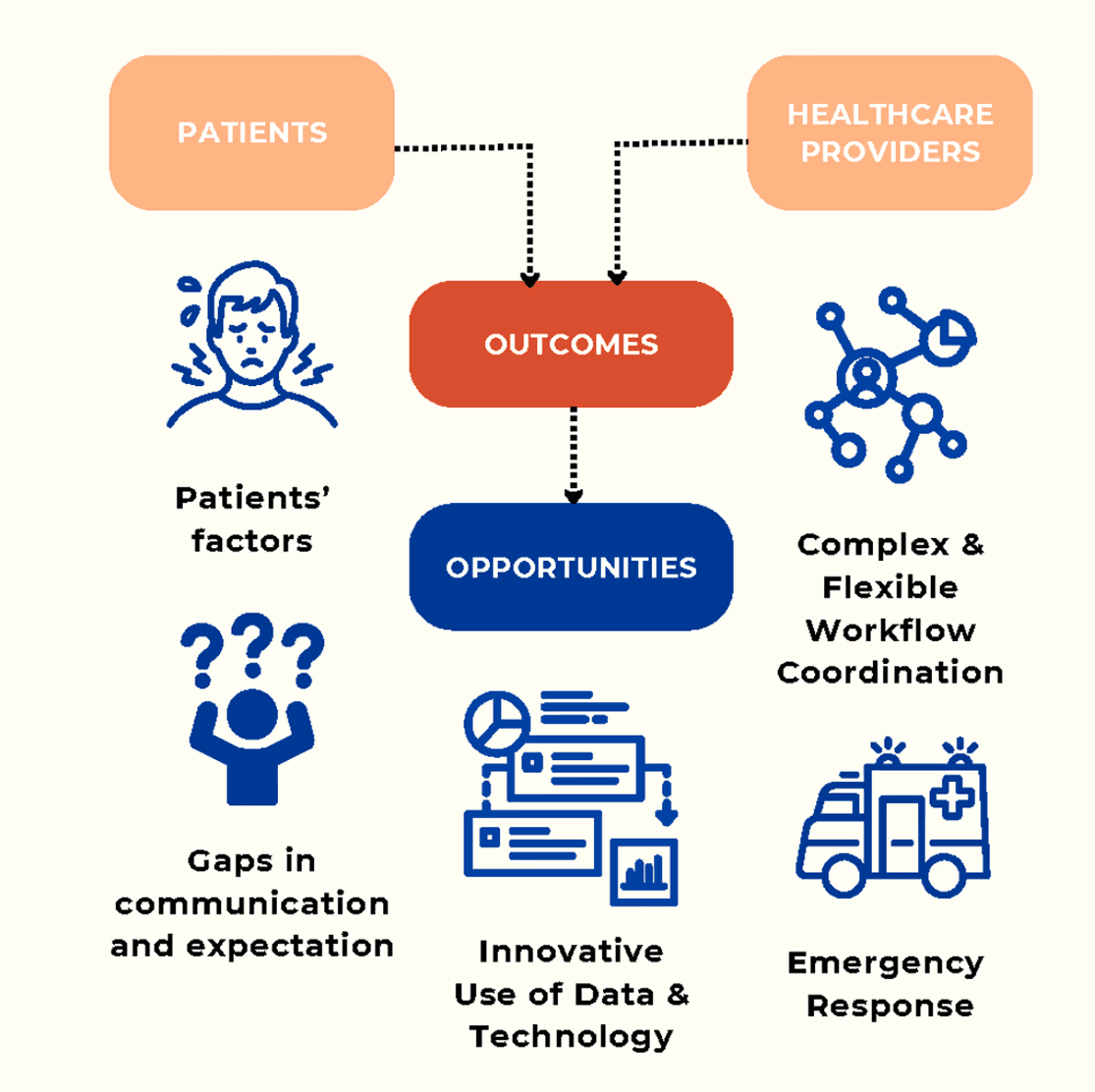
Fig. Key pain points and design opportunities: communication gaps, complex workflow coordination, and emergency response are the three pressure points where design can intervene.
The research pointed to a consistent pattern across all bottlenecks: coordination at CVIC was held together by people, not systems. Clinical staff absorbed what the tools did not handle. Three insights framed the design directions:
Coordination is fragile and reactive
Patient status needs to be visible without requiring manual input to maintain it
Technology should reduce coordination overhead, not add to it
Proposed nine design directions across four themes
Patient communication: pre-visit information and digital checklists to reduce incoming queries and set clear expectations before arrival
Tracking and notifications: real-time patient status visible to staff and families; sensor or check-in triggers to automate status updates rather than relying on manual input
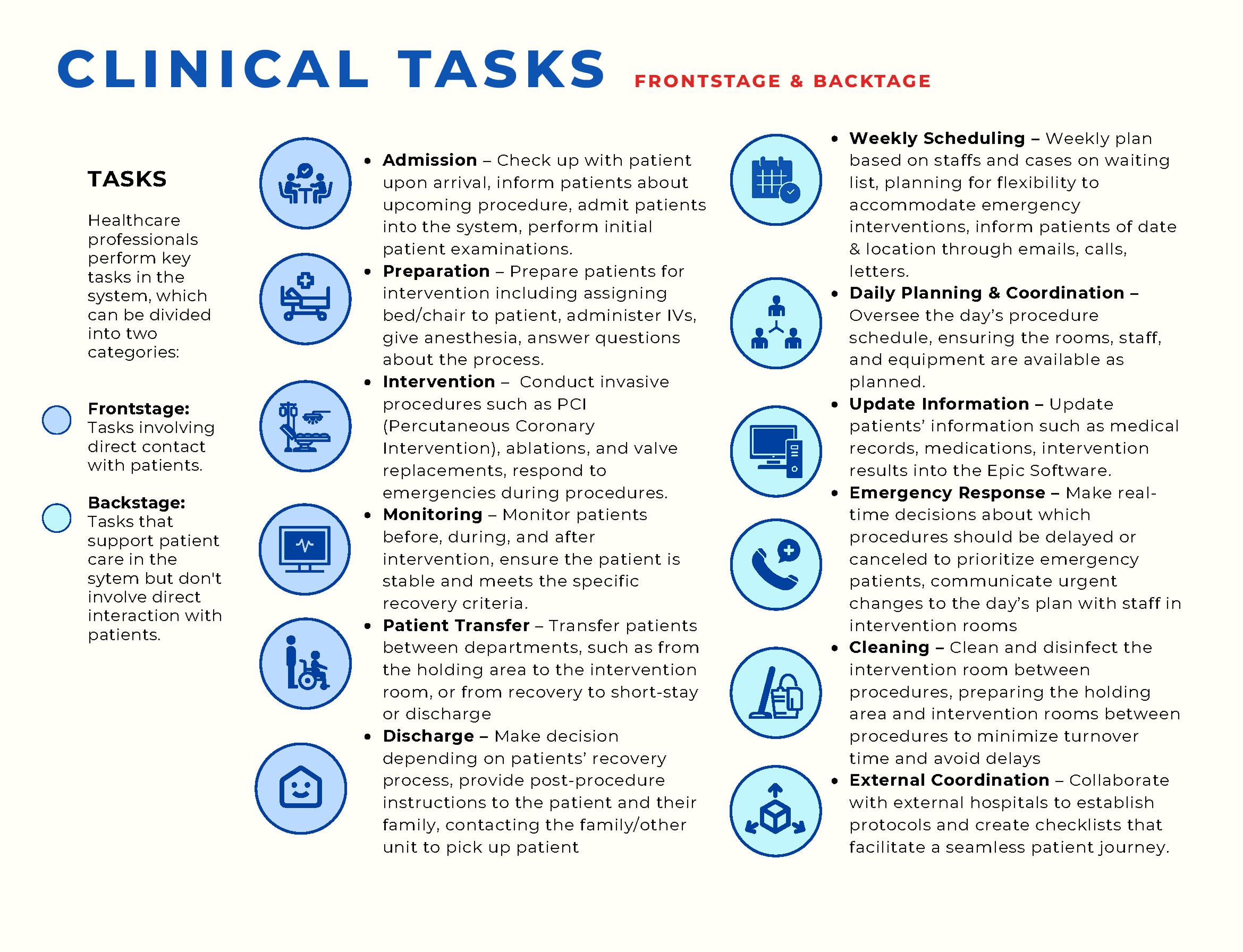
Task and flow management: clinical staff receive task-specific mobile notifications instead of monitoring screens; a dedicated logistics coordinator absorbs coordination work currently distributed across clinical staff
Recovery and family support: digital tools for families to track patient progress and communicate during holding and recovery
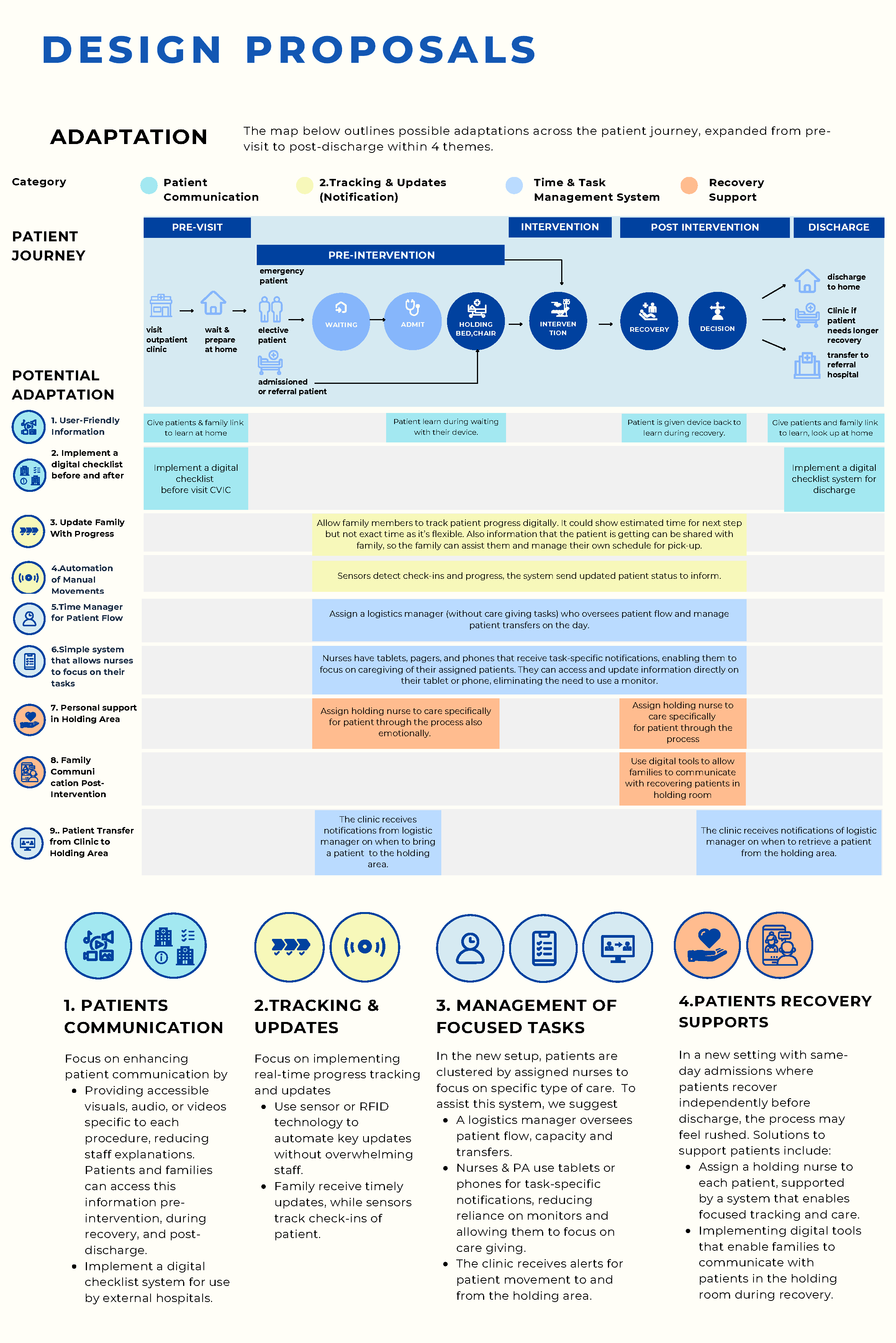
Fig. Nine proposals mapped across the full journey in four themes: patient communication, tracking and notifications, task and flow management, and recovery support.
Expected outcomes
For clinical staff: Manual status tracking and inter-room calls would be reduced. Task-based notifications would allow staff to focus on patient care rather than logistics. A dedicated logistics coordinator role would absorb coordination overhead currently sitting with clinical staff.
For patients and families: Clearer pre-visit expectations would reduce anxiety and incoming clarification calls. A family update system would reduce isolation during holding, and reduce families as a source of interruption for staff.
Limitation: Concepts were validated through stakeholder review with clinical staff and a patient engagement workshop. Direct observation was limited to the admission phase. These were design recommendations for the CVIC expansion, not a shipped system.
Categories
Categories:
Project Details
My Role
Service Design
Team:
Pitshaya Chonato, Puck van der Veer
Affiliation:
Amsterdam UMC, TU Delft, Design in Health course


